
In part two of "Normal pressure hydrocephalus: the "grown-up" version of an under-recognized problem" we looked at what causes normal pressure hydrocephalus or NPH and how it is diagnosed. In part three we will explore what treatment options are available.
V. What treatment options are available?
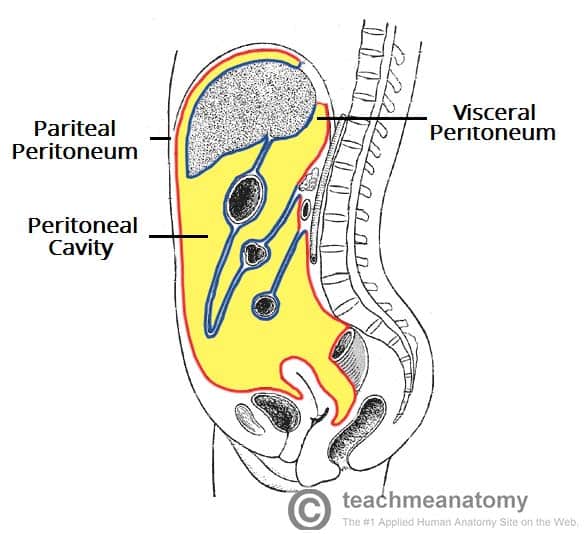
 Just like its counterparts acquired hydrocephalus and congenital hydrocephalus,the only available treatment is surgical implant of a shunt (pictured at right). Most shunt systems consist of three (3) components: 1) A collection catheter (the ventricular catheter in the picture at right); 2) A valve mechanism that controls how much CSF flows through the system; and 3) An exit catheter (the peritoneal catheter in the picture at right) to drain the CSF to another part of the body where it can be absorbed -- in this instance, the peritoneal cavity in the abdomen. In most cases of NPH, the most common shunt implant is a peritoneal shunt and the most commonly used system is the ventriculoperitoneal system which goes from the cerebral ventricle to the peritoneum. Alternatively, the drainage catheter can also be placed in a vein that leads to the heart known as a ventriculoatrial or VA shunt. With either system, once the implant surgery is completed, all components of the shunt system are entirely under the skin.
Just like its counterparts acquired hydrocephalus and congenital hydrocephalus,the only available treatment is surgical implant of a shunt (pictured at right). Most shunt systems consist of three (3) components: 1) A collection catheter (the ventricular catheter in the picture at right); 2) A valve mechanism that controls how much CSF flows through the system; and 3) An exit catheter (the peritoneal catheter in the picture at right) to drain the CSF to another part of the body where it can be absorbed -- in this instance, the peritoneal cavity in the abdomen. In most cases of NPH, the most common shunt implant is a peritoneal shunt and the most commonly used system is the ventriculoperitoneal system which goes from the cerebral ventricle to the peritoneum. Alternatively, the drainage catheter can also be placed in a vein that leads to the heart known as a ventriculoatrial or VA shunt. With either system, once the implant surgery is completed, all components of the shunt system are entirely under the skin.The shunt valve is a critical component of the system and the design that has been in use is the differential pressure (DP) valve. It operates by the valve opening when the (fluid) pressure at the inlet of the valve exceeds the (fluid) pressure at the outlet by a preset amount. In adults with hydrocephalus, the valve is sometimes overwhelmed by the effects of gravity, leading to the drainage of too much CSF. The common name for this over-draining is siphoning. In some cases the patient is asymptomatic while others experience headache or nausea while in an upright position. In extreme cases it can also result in so much CSF being drained that it causes subdural hematoma. To counteract this problem, valve mechanisms have been designed that incorporate both anti-siphoning and gravity-compensating mechanisms. The anti-siphoning mechanism component is triggered by a change in the CSF pressure while the gravity-compensating mechanism is triggered by postural changes.
For additional information:
NPH booklet
No comments:
Post a Comment